Balancing the Equation of Quarantine (Self Isolation), Testing, Mental Health and Economics
5th September 2020 (Sat Japan Time)
A) QUARANTINE (SELF-ISOLATION) in JAPAN vs. SINGAPORE
I am nearing the end of my 14-day self-isolation in Japan. So far, the experience has been extremely positive compared to my Stay-Home Notice (SHN) experience in Singapore back in March 2020.
Looking back at my quarantine experience in Singapore, I must admit I felt quite depressed during that time. The main reason was the restricted movement—I couldn’t leave the quarantine location (my grandmother’s flat) at all. The only movement allowed was between my bedroom, the kitchen, and the bathroom for basic necessities.
I received a call for a spot check almost every day from the Immigration & Checkpoints Authority (ICA), and I had to upload a selfie along with a picture of my quarantine environment to a specific government portal. Additionally, I had to click on a GPS tracker link sent to me via SMS to confirm I was at the quarantine location at all times.
In summary, the entire experience felt more like "house arrest."
In contrast, the experience in Japan was much more pleasant. Upon arrival at Narita Airport, I was guided through various stations, each with a specific purpose. I was briefed on the rules and trusted by the Japanese authorities to fulfill my responsibilities as a responsible citizen. Every passenger was required to take a saliva PCR test at designated booths, with results available within 90-120 minutes.
While waiting for the results, passengers were allowed to work on their laptops and were free to self-serve mineral water and traditional Japanese snacks (such as dorayaki and senbei), embodying the Japanese spirit of omotenashi (hospitality).
After receiving my test results, I proceeded to the immigration counter, passed through customs, and collected my luggage as usual. A "quarantine" bus was provided for those of us booked at hotels near Narita Airport. I was then transferred to my hotel and checked in without issue.
The hotel staff, trained to handle returnees like me, explained the rules in detail. As part of the protocol, I was required to take my temperature twice a day at the reception—once in the morning and once at night. In case of an emergency, an official contact number was provided.
My movements were restricted to the hotel vicinity, which included a large parking lot where I could jog, walk, and do sprints. The gym was open 24 hours, breakfast was available from 6 am to 10 am, and there was a 24-hour convenience store in the lobby.
Huge carpark where I did my running & sprinting

100m sprint at the carpark

The food at the breakfast buffet was protected by the "highest level of security"—every item was individually wrapped, except for the bananas and oranges.

For lunch and dinner, I could either order from the regular room service à la carte menu or choose from a "cheaper" customized menu specially designed for returnees like me who are staying for 14 days. The menu was divided into four sections (A, B, C, and D), with a new selection each week. The prices were reasonable, ranging from 1,000 JPY to 1,500 JPY, which is typical for Japan when dining at franchise restaurants (though not comparable to the 350-500 JPY beef rice bowls, or gyudon, at Yoshinoya).
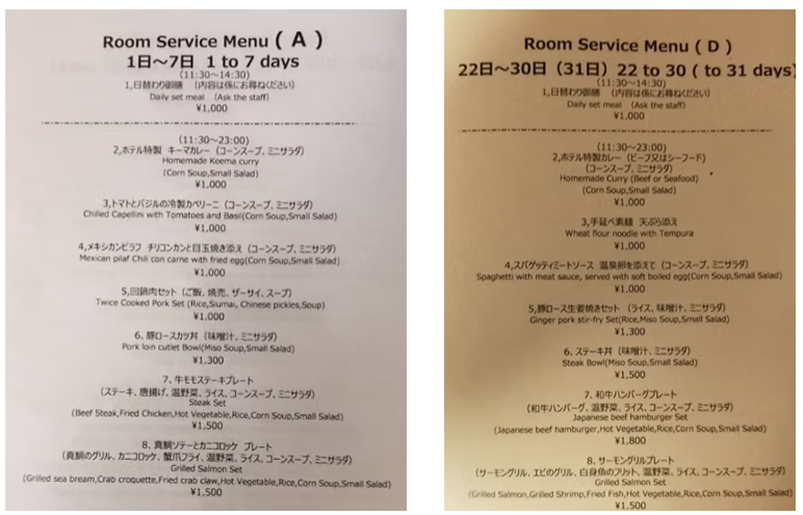
Number 8 on Menu A

Another option was to purchase a bento or food from the 24-hour convenience store in the lobby.

Housekeeping is available, but the reception asks for the specific time and items to be serviced when you take your temperature in the morning. This helps ensure that all housekeeping staff are properly tracked.
As part of the hotel's safety measures, hand sanitizers are available everywhere— in the elevators, reception, lobby, breakfast area, gym, restrooms, etc.
As my residency is registered with Chiyoda Ward in Tokyo, I am required to send my daily temperature recording to the Chiyoda Ward COVID-19 taskforce email, except on weekends.
Additionally, from the 8th to the 12th day of quarantine, the person in charge called me to monitor my health condition.
In summary, compared to my experience in Singapore, the self-isolation process in Japan was far more pleasant and, in my opinion, “humane.”
Unless one is a hikikomori (a person who withdraws from society), being unable to leave your room for 14 days is a real challenge to both physical and mental health.
Reference article on the life of a hikikomori:
In Singapore, authorities seem to assume that everyone will break the rules, and the calls are often filled with suspicion. There was even a time when a “Safety Officer” asked me with contempt whether I was truly at home serving quarantine. I challenged him to come to my place personally to verify it. This mindset is understandable, as Singapore transitioned from a third-world country to a first-world nation largely through fines, penalties, and strict disciplinary actions—built on a foundation of fear.
In contrast, Japan's approach is different. The calls are made with the intention of monitoring health, based on the trust that responsible adults, as part of society, will do the right thing.
To be honest, the approach, tone, and questions asked during these calls can greatly affect one's mood and mental health during quarantine. Safety officers should remember that those placed under quarantine have not committed any crimes; they are simply fulfilling their duty as responsible citizens, as required by the authorities.
B) UNDERSTANDING IMMUNITY, CASE FATALITY & MENTAL HEALTH
As a regular gym-goer, the quarantine in Singapore posed a significant challenge—I lost at least 3-4 kg, including a considerable amount of fat and muscle, during the lockdown.
My body fat percentage dropped to 12%, and unfortunately, I also experienced muscle loss.
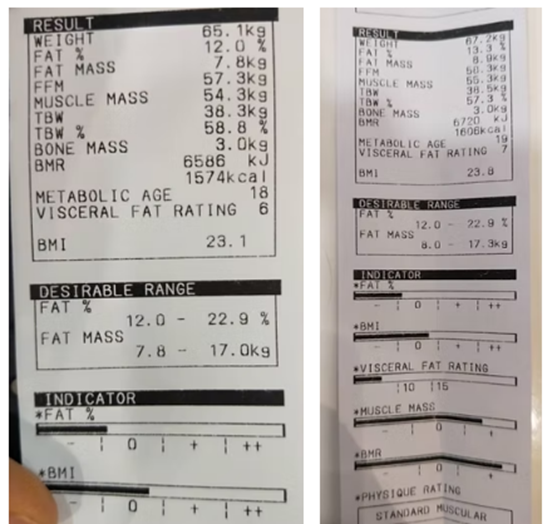
After returning to the gym for a month, I gained back 2 kg of weight, including 1 kg of muscle. I’m continuing to work towards my goal weight of 68-69 kg with more muscle mass.
IMMUNITY
According to common knowledge (as referenced in the Forbes article below), there are 4 key elements to boost the immune system:
- A balanced diet, rich in vitamins and nutrients
- Regular exercise and breathing fresh air
- Sufficient rest
- Mental well-being: staying in touch with friends and family
- Hygiene: (This is my addition, not in the Forbes article)
It’s a no-brainer to conclude that one of the keys to fighting COVID-19 is boosting the immune system.
However, the question remains: Are the quarantine policies in place in different countries supporting their populations in doing so?
Assuming the advice in the Forbes article is correct, how many countries’ quarantine policies actually align with these criteria?
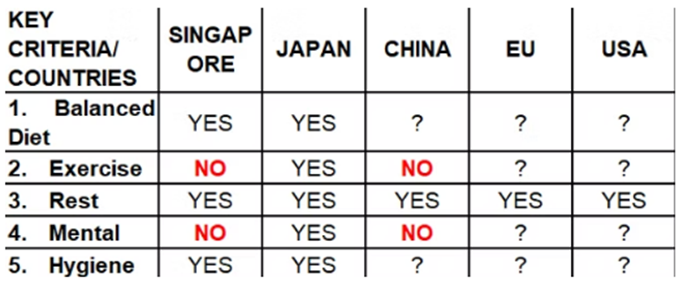
Note: In Singapore's case, I cooked healthy meals at my grandmother’s home, so I would rate it as "YES" for diet. However, I’m unsure about the food served at designated quarantine hotels. For "Mental," I gave a "NO" because I wasn’t allowed to step outside for fresh air, let alone exercise.
This brings me to my second point: CFR – Case Fatality Rate. How fatal is COVID-19 to justify the current quarantine policies?
CASE FATALITY RATE (CFR)
What is the Case Fatality Rate?
The acronym CFR refers to the proportion of deaths among all individuals diagnosed with a particular disease, commonly known as the "case fatality rate."
For those interested in the formula, here’s the link from the WHO on how to calculate the fatality rate: https://www.who.int/news-room/commentaries/detail/estimating-mortality-from-covid-19
How fatal is COVID-19?
· Due to the novel nature of this virus and the complications, it is rather difficult to estimate the CFR.
· There are many factors to consider and one of the key factors is underlying health conditions.
https://ourworldindata.org/mortality-risk-covid#interpreting-the-case-fatality-rate
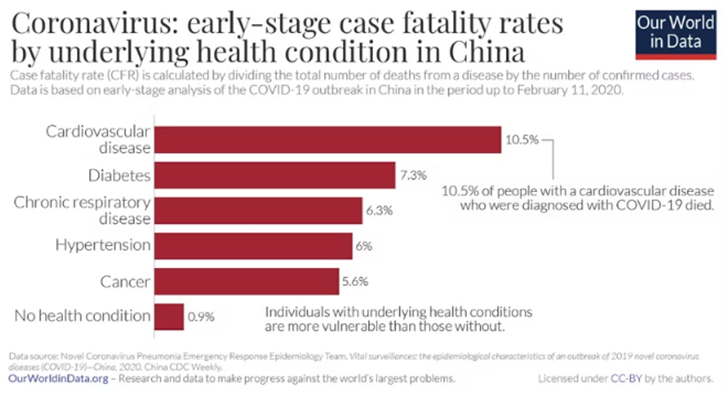
It is clear that patients with cardiovascular disease are 10 times more likely to die from COVID-19 than those without any pre-existing health conditions.
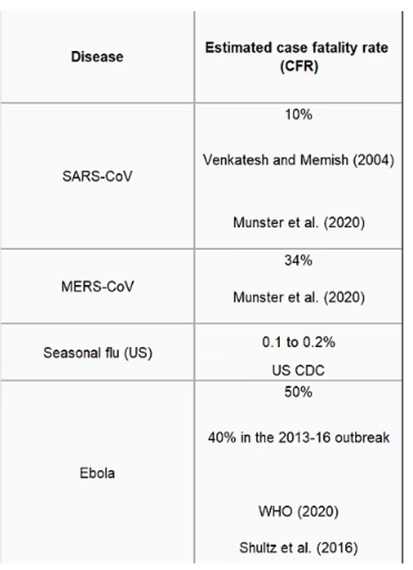
How does the fatality of COVID-19 compare to other viruses?
Source: https://ourworldindata.org/mortality-risk-covid
COVID-19 is less fatal compared to MERS and SARS but more deadly than the seasonal flu in the USA.
However, based on what the world has witnessed in the past 8 months – it is highly infectious and spreads much more easily.
Luckily, COVID-19 is also a relatively mild virus for the fit and healthy – just look at the examples of professional athletes who contracted and recovered from the virus.
Also, many fit and healthy professional athletes show little or no symptoms at all. In fact, about 30% of the infected are founded to be asymptomatic which makes detecting a challenge without testing.
Football: I’m fine, says Juventus player Rugani after testing positive for coronavirus

PUBLISHED
MAR 12, 2020, 6:25 AM SGT STRAITS TIMES SINGAPORE
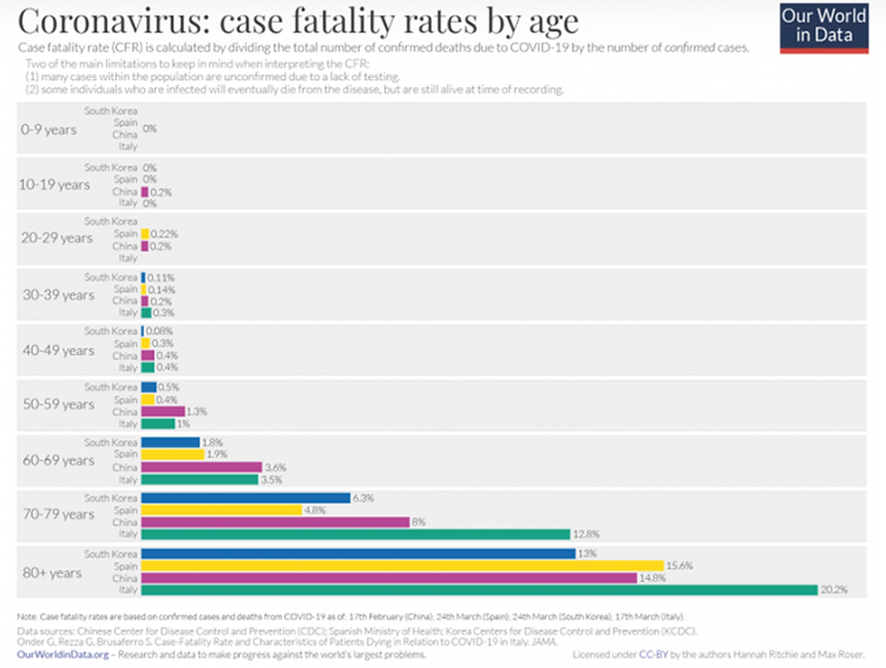
The second major contributing factor is age – as one ages, their immune system deteriorates, hence the higher CFR.
This logically puts someone who is 80+ years old with pre-existing health conditions at the highest risk.
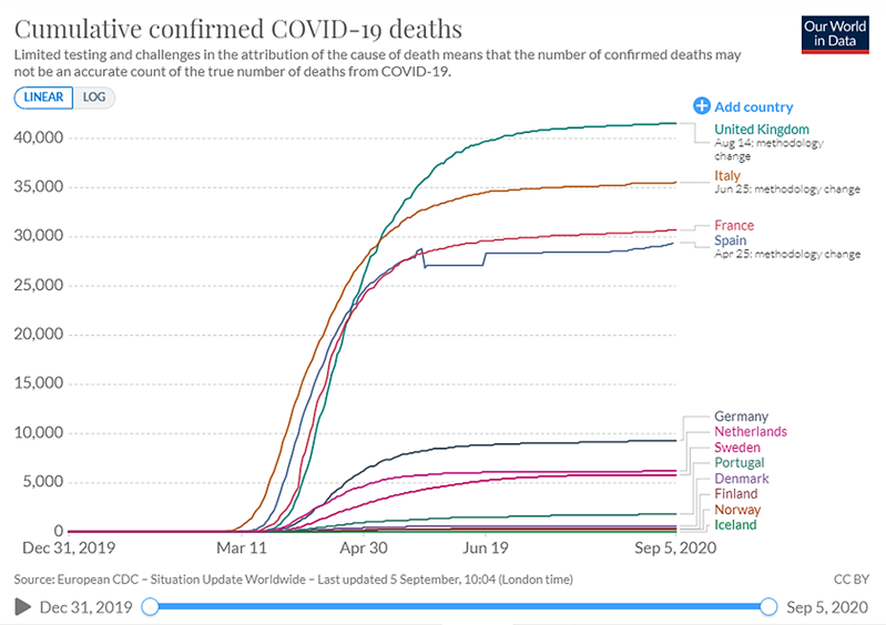
The third major factor is the difference between lockdown and no lockdown. I will use Scandinavia as a bloc to demonstrate my point – because the income equality gap is small and healthcare quality [national health insurance coverage] is high in Nordic countries – making comparison easier and fairer.
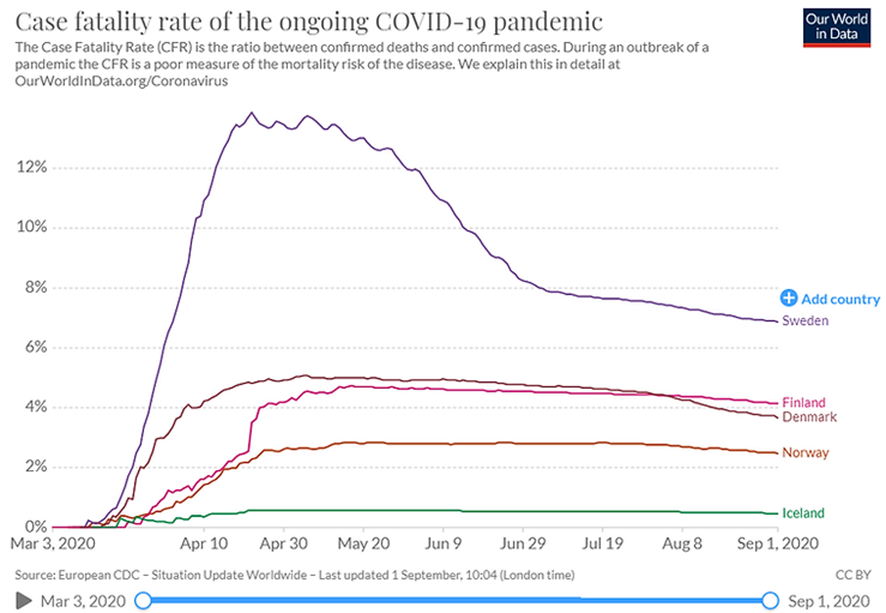
Gap in CFR
Source: https://ourworldindata.org/mortality-risk-covid
Note: Countries like Russia, the USA, and China are not ideal examples for comparison due to their vast land sizes, large populations, and decentralized policies implemented by various states and cities.
Sweden did not implement a lockdown, instead opting for a "herd immunity" policy, in contrast to its Nordic neighbors. During the peak, Sweden's CFR rose as high as 14%—almost three times higher than Denmark and Finland, where the CFR remained below 5%.
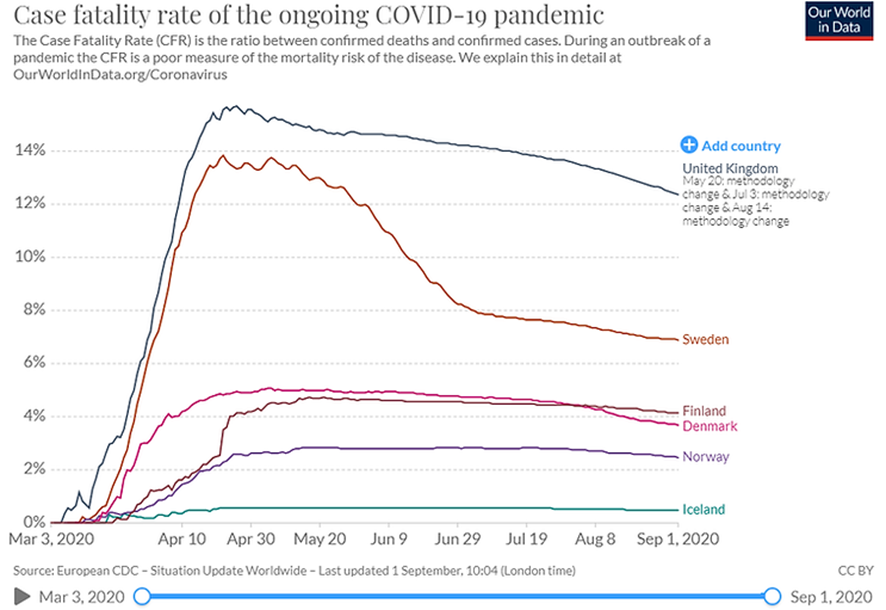
Now, let’s add the UK to the equation. Interestingly, the UK was initially encouraging the "herd immunity" concept until Prime Minister Boris Johnson and Health Secretary Matt Hancock both tested positive for COVID-19 on March 27, 2020, and death rates began to rise. It was then that the UK decided to implement a "mild lockdown." Notably, the UK's trend between March and June was similar to Sweden’s.
Some may argue that Belarus also had no lockdown. Let’s take a look at the data from Belarus.
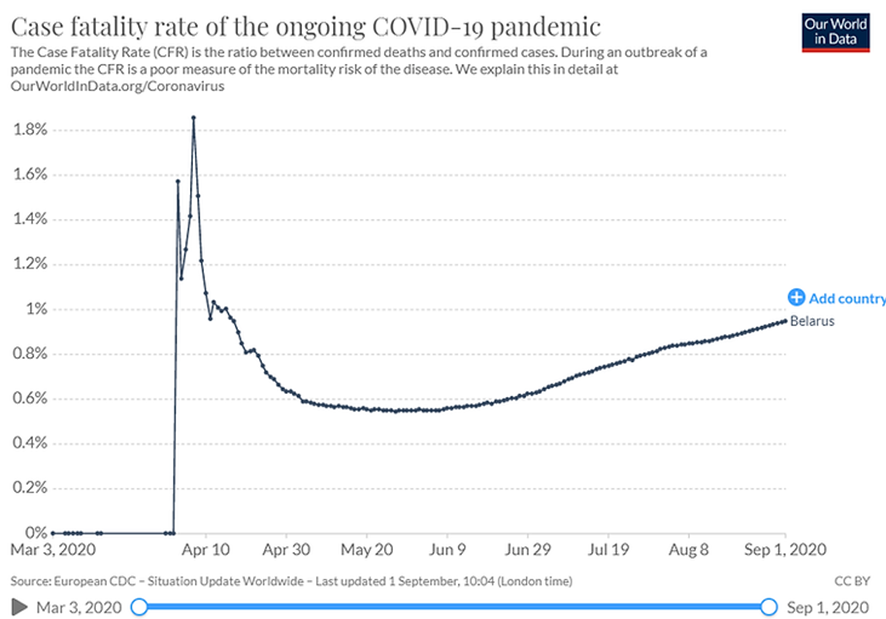
Sure, the CFR appears to be around 1% to 2%, but there are currently huge protests in Belarus against President Lukashenko over election fraud. Which country, amidst political demonstrations, would actually conduct widespread COVID-19 testing? Additionally, can we trust data from a country whose president claimed he won the election with 80% of the vote?
Beyond lockdowns, measures like masking, social distancing, and handwashing also play a significant role in controlling infection levels.
The fourth factor is the quality and availability of healthcare. However, quantifying "healthcare quality" is challenging, so I’ll leave that out of this discussion.
For a more constructive and solid analysis, data on healthcare coverage would be necessary. For example, 90% of the population in Germany is covered by the German National Healthcare Insurance. Additionally, evaluating healthcare quality is largely subjective—it can range from the availability and quality of medical equipment to the number of physicians per 1,000 people, the expertise of medical staff, and the number of virology-trained physicians. After all, a neurosurgeon wouldn’t be very helpful in the context of COVID-19, would they?
Now that we understand COVID-19 is highly infectious but has a relatively low CFR (compared to SARS in 2002-2004), especially for healthy individuals, let’s examine the quarantine policies currently in place.
C) QUARANTINE POLICIES – ESSENTIAL OR EXCCESSIVE?
To begin, we need to recognize that 14-day quarantine/self-isolation is the general guideline. However, each country implements its own quarantine policy.
Let’s start with China, where the outbreak originated. In most cities, 14 days of quarantine is the norm. However, Beijing implemented a more extreme policy. Initially, travelers had to alight at an airport near, but outside of Beijing—such as Tianjin or Dalian. Quarantine would take place at a designated hotel for 14 days. Afterward, they would be allowed to enter Beijing, but must quarantine in their apartment for an additional 14 days, totaling 28 days. This was the original policy when China faced a high number of imported cases.
The situation has changed now. While entry into Beijing is still restricted, travelers must now go through 14 days of quarantine at a nearby city, which includes three PCR tests: the first upon arrival, the second on day 7, and the last on day 14.
Needless to say, individuals are not allowed to leave their rooms at any time during this period.
Singapore’s quarantine policy is similar to China’s, though without the testing. Returnees are now required to quarantine for 14 days, and if they show no symptoms, they can leave without testing. However, Singapore remains firm in its stance of not testing asymptomatic individuals.
The situation in the EU is more complicated, especially since quarantine conflicts with the Schengen Area's principle of free movement. The EU has issued guidelines, but member countries are not required to follow them. If you are traveling from another EU country, no quarantine is required. But if you are traveling from a third country outside the EU, the rules vary from country to country. Below are a few examples as of the time of writing. Please note that these rules are subject to constant change depending on the global infection situation.
If a traveler is from a fellow EU country, the table below does not apply. The regulations only apply to third countries that are on the list of 15 approved nations allowed to enter the EU.
Among EU countries, Poland has the most relaxed policy, while Hungary is the strictest. Please note that PCR test requirements are largely dependent on the airline. For example, while Poland does not require a PCR test for entry, travelers transiting through Emirates Airlines will need to present a PCR test result before boarding.
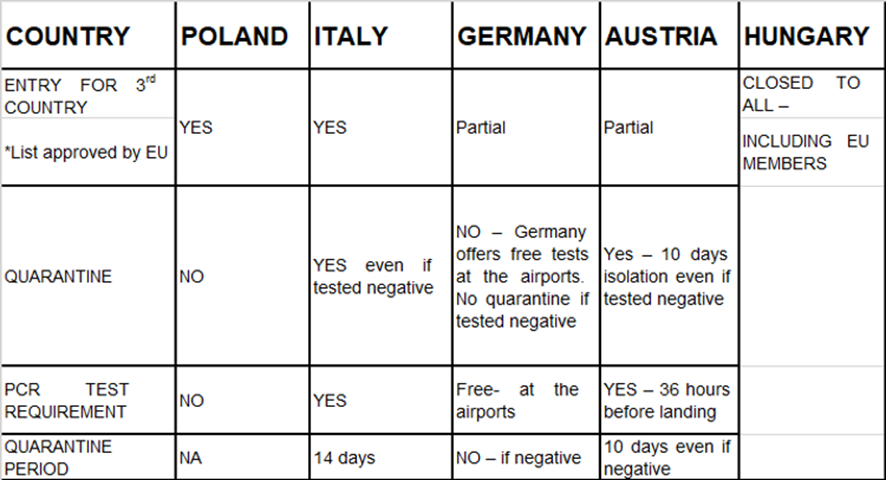
An interesting point is that politicians (typically those involved in foreign affairs) or essential business travelers are exempt from self-isolation if their test results are negative.
This raises a couple of questions: Why are politicians and business travelers, who are humans just like regular travelers, not required to self-isolate while others are, even with a negative test result? Our DNA and genome cannot differ that significantly, can they?
The second question is: Are authorities not confident in the accuracy of the tests? If someone tests negative, could they suddenly test positive after leaving the airport?
This leads to a third question: If authorities are not confident in the test kits or testing methodologies, how can we trust the vaccines they approve? It is common knowledge that developing a vaccine is far more complex than creating a test.
In summary, the quarantine policies send mixed messages. On one end, we have the extreme, draconian quarantine practices in China, and on the other, the ambiguous free movement policies within Europe. An EU national is no less susceptible to the virus than a third-country national, so why the double standard? If the test result is negative, why can't a third-country national move freely, just like an EU national? Unless, of course, the authorities do not trust the accuracy of the tests.
D) TESTING, BORDER-OPENING & THE ECONOMY
This pandemic has impacted global travel and various industries both positively and negatively. The healthcare and logistics industries are experiencing bumper years like never before while the retail, travel and banking industry are suffering tremendously.
Politicians are leveraging on COVID-19 one way or another to fuel their political agenda – sometimes in a despicable manner. One of the most recent examples involve the recent retweet by US President, Donald Trump about the 6% data released by the CDC. Source:https://www.forbes.com/sites/brucelee/2020/08/31/twitter-removes-claim-about-cdc-and-covid-19-coronavirus-deaths-that-trump-retweeted/#238919443178
There are already many conspiracy theories going on – and a misleading retweet by the US President will only cause more confusion among a nation that loves conspiracy theories. For those who do not look deeper beyond the numbers, or are not trained in data interpretation, the retweet or headlines could have very serious impact. It will be interesting to see how the politicians [especially in USA] manipulate COVID-19 related figures in the upcoming months leading to the November election.
In general, the message and measures have been mixed on both ends of the spectrum – extreme draconian measures, “herd-immunity” concept, half-witted American students throwing COVID parties, conspiracy theorists linking COVID-19 to 5G technology, and those calling the virus a total hoax etc.
Even the awareness on how the virus spreads is not aligned despite evidence proving that COVID-19 could be transmitted by aerosols (see link below). This means that smoking, shisha bars, indoor dining with poor ventilation are potentially hotbeds for the virus.
Source: https://time.com/5883081/covid-19-transmitted-aerosols/
Testing Methodology
The testing methodology and border-opening policies are not aligned and standards are ambiguous too. Example: for nasal swab tests, do we use a different swab for each nostril or the same swab for both nostrils? Do we take a nasal swab specimen + an oral swab specimen from the same patient?
Based on scientific principle, any variable might impact results and until the testing standards are aligned, there will always be the possibility of debatable outcomes. Personally, I have taken three tests to date and none of these methodology is identical, albeit all negative.
Test Analysis
At the moment, the PCR test is considered to be the “gold standard” benchmark.
However, there are two conflicting views according to New York Times and Japan Times.
The New York Times claimed that the current analysis is overly-sensitive, while the Japan times claimed that the current PCR test are NOT sensitive enough – producing 30% false negatives.
Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.
“The standard tests are diagnosing huge numbers of people who may be carrying relatively insignificant amounts of the virus” (see article below).
In contrast, according to the Japan Times, the current PCR test is NOT accurate enough:
“While PCR tests are generally regarded as highly accurate, the true accuracy rate is about 70 percent, which means about 30 percent of infected people receive false-negative results.” Japan Times, 1 September 2020
Source:https://www.japantimes.co.jp/opinion/2020/09/01/commentary/world-commentary/reopen-national-borders/
Are New York Times and Japan Times making this statement based on the same empirical testing methodology and analysis? With the current amount of information, we cannot conclude unless we look into the methodology and the technical evaluations behind those respective comments.
Assuming that New York Times is correct, the problem with the current analysis is as follows:
1. Cycle threshold is set between 37-40
- COVID-19 is a RNA virus and needs to be converted into DNA and duplicated multiple times during analysis to detect the virus.
- If a patient is a super-spreader, virus will be detected in the specimen within 10-20 cycle threshold; the more cycle threshold required to detect the virus, the less contagious the patient is.
- The current 37-40 cycle threshold in the USA is considered to be relatively more conservative, and overly-sensitive by New York Times.
2. Amount of virus is not recorded – waste of precious data and testing
3. Risk: as the incubation period proceeds, the viral load might increase depending on the day the patient is infected, so lowering the cycle threshold might not be wise.
Testing Policies
The testing policies have become highly polarized. On one extreme, South Korea is conducting mass testing, while at the other end of the spectrum, the President of Belarus has suggested that citizens drink vodka and return to work.
In Asia, there is a developed nation with a high GDP per capita and one-tenth of Korea’s population size, yet it refuses to test patients without symptoms, even as reports show that 30% of those who test positive are asymptomatic. Japan, initially focused on protecting its Olympic ambitions, ultimately faced a surge in infections after the Olympics were postponed.
Testing Policies in Different Countries
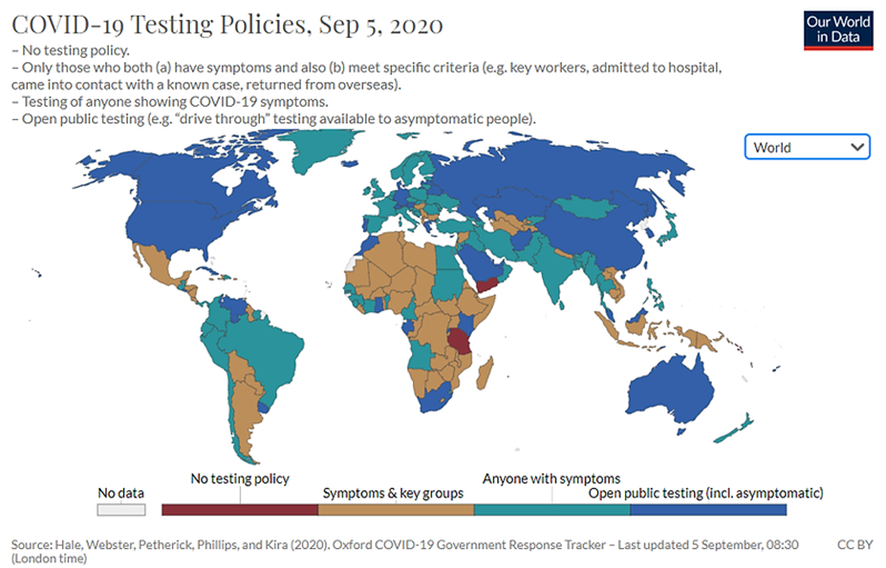
Source: https://ourworldindata.org/coronavirus-testing#testing-vs-gdp-per-capita
Germany’s Decision on Testing
Unsurprisingly, the Germans are one of the most efficient and effective with their testing measures and have one of the lowest death rates in Europe.
- Testing is free for ALL
- Testing is AVAILABLE at all major German airports
- Test results are FAST – within 24 to 48 hours
- SOLIDARITY AGAINST A COMMON ENEMY: Germany disseminated a blueprint for a test to all public and private hospitals and laboratories as soon as possible.
- HEALTHCARE SYSTEM FOR THE PEOPLE: 90% of Germans are covered by national insurance
- GOVERNMENT LEADERSHIP: by May, it was mandated that all insurance companies have to cover cost of testing
- TEST ALL (including asymptomatic)
Source:https://www.nytimes.com/2020/08/05/world/europe/germany-coronavirus-test-travelers.html
OPENING THE BORDERS
In an ever-increasingly inter-connected world, the borders have to resume sooner or later. However, the current regulations and protocols do not provide sufficient “safety” to reopen the borders.
Without the reopening of the borders, a country has to rely on trade (imports and exports) and their domestic market for economic growth, which is somewhat restricted unless the country has a huge domestic market.
One example is China – largest population in the world, huge domestic market and has basically returned to growth – the only country with positive GDP growth in the 2nd quarter of 2020.
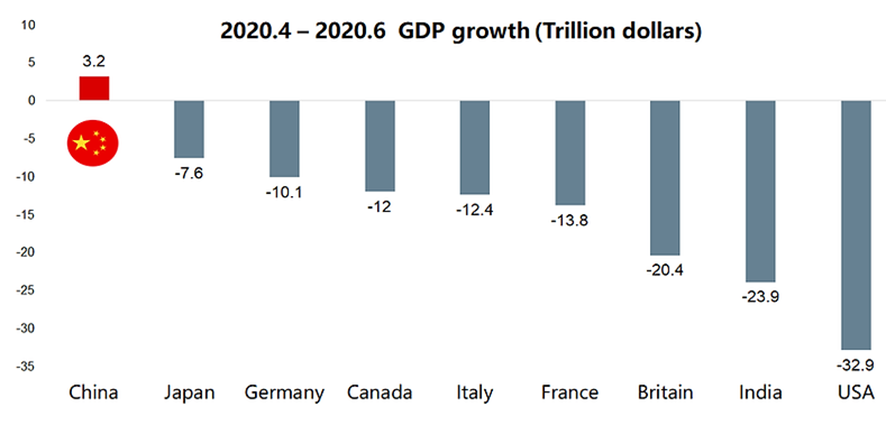
Source: https://www.bbc.com/news/business-53399999
However, most countries are NOT China and are in need of external demand and traffic in-and-outflow for economic growth – in particular the EU Region.
Therefore, the key question will be how to open the borders safely.
E) CONCLUSION & RECOMMENDATION
The pandemic has disrupted many traditional business models and challenged conventional wisdom, behaviors, and ways of thinking. To adapt to this new paradigm, it is essential to remain open-minded, embrace our curiosity, and develop new norms and guidelines to help us navigate the future.
At the core, we need to focus on 3 KEY parameters, and this requires global solidarity more than ever. Personally, I am NOT an advocate for vaccines. My position remains: if authorities are not confident in the testing methods they have developed and cannot even align testing and quarantine protocols, how can they be certain about the effectiveness of vaccines?
Step 1, everyone needs to agree, align and STANDARIZE the following 3 elements:
1. TESTING METHODOLOGY
- Approve a list of testing methodology – example: RT-PCR nasal, oral, and saliva etc.
- For swabs, at least a nasal and an oral specimen from the same patient need to be provided for laboratory analysis.
- A cheaper alternative will be antigen testing – this will be a topic for another day.
2. TESTING ANALYSIS
- Cycle Threshold: decide on the cutoff – 35 or the current 40
- Without the same cutoff cycle threshold, there can never be an apple-to-apple comparison. It also impacts decision-making and longitudinal analysis in the long run.
- Record the viral load for deeper study and analysis; research & development purpose
3. TESTING & QUARANTINE PROTOCOL
- Test ALL including asymptomatic when crossing borders
- Test on Day 1, Day 7 and on Day 14 – total of 3 tests – triple negative.
- Not required quarantine/ self-isolation if test on Day 1 is negative, however monitor health and continue testing on Day 7 and Day 14 until fully cleared. The person has to be socially responsible and remain contactable by the authorities for the next 14 days.
In sum, we are living in unprecedented times and the need for global solidarity has become more important than ever. Instead of divisive politics and international policies, it is time for the world to develop a standardized and safe protocol that could help everyone move forward.
Once the three key elements are in place, borders can reopen safely, and businesses can resume operations, with masking, social distancing, and personal hygiene measures in place to maximize effectiveness.
After achieving Step 1, a shared global database of findings could be established among the CDCs in each country. This would provide valuable insights and allow for continuous system improvement.
In conclusion, we are living in unprecedented times, and global solidarity has never been more crucial. Instead of focusing on divisive politics and fragmented international policies, it’s time for the world to establish a standardized, safe protocol that will help everyone move forward.
AREZZO FOUNDER
HUMPHERY CHEN